How to Use the B12 Protocol (Part 2): Molybdenum and Riboflavin
This blog post is the second of a three-part series on how to use the B12 Protocol. To access Part 1, click here. In this series, we will cover the steps involved in fully implementing the B12 Protocol as a means of improving the Trifecta of health. I will be repeating some information from Part 1 where appropriate.
While there is no single correct order of implementing the vitamin B12 Protocol to repair methylation capacity, redox capacity, and mitochondrial health, this series will describe the most common order of doing it. Doing the steps in a different order is more likely to result in temporary, but unpleasant, side effects as a result of increasing demand for metabolic processes that may require some preparatory steps to be in place.
If you implement all of the steps of the B12 Protocol, it should not have any different result in the end, and in that context, the order is not significant from a final result standpoint. However, to reduce or avoid negative symptoms while improving the components of the Trifecta, it is imperative that you make changes by listening to what your body (and lab testing) tells you. This order is the well-traveled path, if you will.
Here is a succinct biochemical conclusion of what was accomplished by implementing Part 1 of the B12 Protocol:

This is assuming that we are receiving a reasonable amount of vitamin B2 from our diet. The most adequate dietary sources of vitamin B2 include most animal flesh, eggs, and dairy. Step 2 involves supplementing vitamin B2 in order to amplify the effects of Step 1 (depicted in the illustration above) and further activation of FMN through Molybdenum supplementation.
Step 2: Taking Functional Vitamin B2 Status to the Next Level
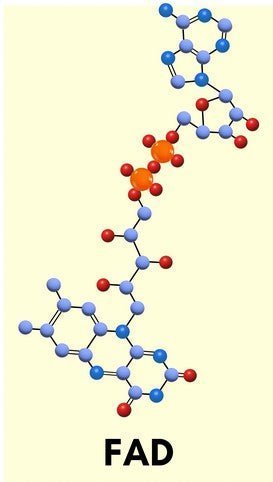
In the cascade of activating vitamin B2 (MTHFR's cofactor), one specific form of vitamin B2 is required: Flavin Adenine Dinucleotide, which is more commonly referred to as FAD.

FAD is produced by an enzyme that takes another active form of vitamin B2 (Flavin Mononucleotide, FMN) to create FAD. The enzyme FAD Synthase accomplishes the task with the assistance of molybdenum cofactor, by attaching the AMP portion of an ATP molecule to FMN. This results in the active form of vitamin B2 used by the famous MTHFR enzyme.
MTHFR has received a lot of attention over the past decade or so due to its role in the methylation cycle. Despite what many of the early biohackers were saying about MTHFR genetic variants (they prefer the term "mutation" because that term has a more dire tone), these single nucleotide polymorphisms, or SNPs (pronounced "SNIPs"), do not radically change a person's ability to methylate and they certainly do not doom the methylation cycle to failure.
Some important context to consider is that 80% of the human population has one or more of the supposedly pathogenic SNPs, making them more accurately "variants". While these SNPs may decrease the efficiency of MTHFR somewhat, our body uses epigenetic regulation to upregulate or downregulate genetic expression, meaning if the body senses that the reaction controlled by MTHFR is not happening fast enough, transcription can be upregulated to account for this difference. This process of upregulation and downregulation is called "epigenetic regulation" and is dependent in part upon methylation capacity.
This is why at Spectrum Sciences, we emphasize methylation capacity over what some of the early biohackers used to promote, which amounted to giving "a supplement for a SNP". In the latter approach, a practitioner might look at a genetic SNP report, see which SNPs were reported, and come up with a list of supplements the person would supposedly need because of their broken genetic machinery. This method has its place when genetic information is used to add context to functional testing, but when used in a less nuanced manner, it is mostly a waste of time and money. We do not believe there is any need to know one's MTHFR genotype for the B12 Protocol to be used successfully.
The B12 Protocol, in contrast to the "supplement for a SNP" method, is designed to maximize the body's methylation capacity while simultaneously fixing redox capacity and mitochondrial function, so that the body can make use of epigenetic regulation through its own intelligent design to keep these enzymes working at maximal output. We have not been able to find an association between nutrient dosage and genotype.
The role of Molybdenum
As mentioned in the description of how FAD is produced, the enzyme responsible requires a special cofactor called "molybdenum cofactor", and as the name suggests, molybdenum is incorporated into this molecule. Molybdenum is represented in this model by the teal colored sphere.

Damaged or inflamed guts may not absorb adequate molybdenum from the diet to keep molybdenum cofactor production at levels necessary for optimal FAD production. This is why many people may benefit from use of Molybdenum Oil at this stage in the protocol. With thyroid hormone production ramped up and the ensuing increase in FMN production taking place, the body then is going to require more molybdenum to proceed with this chemical cascade.
With the additional provision of adequate vitamin B2, FAD production can be optimized.
So which is first, Molybdenum or Vitamin B2 supplementation?
Most people seem to add Molybdenum Oil first, followed by Vitamin B2 (contained in Protocol Support multivitamin) approximately 1-2 weeks later. This has more to do with convention and less to do with logic. You can experiment with adding them in the opposite order, or even simultaneously. I will provide a few examples of ways to implement Step 2.
Waiting 1-2 weeks between dosing adjustments is suggested based on how long it takes most people to feel the effect of a particular nutritional change on their mind and body. By allowing enough time to become conscious of the effect of a change, it gives the user a better understanding of how each product impacts them, which can be used to inform dosing.
For those who prefer a visual aid, your progression can take on a few different approaches, depending on how you respond.
Cautious approach #1 (alternating molybdenum titration and B2 titration):
|
|
Molybdenum (drops) |
B2 (mg) |
|
Week 1 (daily) |
1 |
0 |
|
Week 2 (daily) |
1 |
3-5 |
|
Week 3 (daily) |
2 |
3-5 |
|
Week 4 and Thereafter (daily) |
2 |
6-10+ |
*note that each capsule of Protocol Support contains 3.33mg of vitamin B2, and may be used to supply this nutrient
Cautious approach #2 (molybdenum titration, followed by B2 titration):
|
|
Molybdenum (drops) |
B2 (mg) |
|
Week 1 (daily) |
1 |
0 |
|
Week 2 (daily) |
2 |
0 |
|
Week 3 (daily) |
2 |
3-5 |
|
Week 4 and Thereafter (daily) |
2 |
6-10+ |
Quicker approach (simultaneous titration of molybdenum and B2):
|
|
Molybdenum (drops) |
B2 (mg) |
|
Week 1 (daily) |
1 |
3-5 |
|
Week 2 and Thereafter (daily) |
2 |
6-10+ |
Some people who struggle with getting their ft4 and/or fT3 values to increase in response to Iodide and Selenium may wish to first add Protocol Support (which includes vitamin B2) for the antioxidant benefit, which may allow more iodide uptake by the thyroid. An example of that strategy can look like this:
Resistant Thyroid approach #1 (alternating Protocol Support titration and Molybdenum Oil titration):
|
|
Protocol Support (capsules) |
Molybdenum (drops) |
|
Week 1 (daily) |
1 |
0 |
|
Week 2 (daily) |
1 |
1 |
|
Week 3 (daily) |
2 |
1 |
|
Week 4 and Thereafter (daily) |
2+ |
2 |
Resistant Thyroid approach #2 (Protocol Support titration, followed by Molybdenum Oil titration):
|
|
Protocol Support (capsules) |
Molybdenum (drops) |
|
Week 1 (daily) |
1 |
0 |
|
Week 2 (daily) |
2 |
0 |
|
Week 3 (daily) |
2 |
1 |
|
Week 4 and Thereafter (daily) |
2+ |
2 |
Resistant Thyroid approach #3 (Simultaneous Protocol Support titration and Molybdenum Oil titration):
|
|
Protocol Support (capsules) |
Molybdenum (drops) |
|
Week 1 (daily) |
1 |
1 |
|
Week 2 and Thereafter (daily) |
2+ |
2 |
As explained in Part 1 of this series, while the quicker approach is appealing from a time-saving perspective, it removes the ability to feel the effect of Molybdenum Oil and B2 in isolation from each other. If you experience a negative reaction while following this time-saving approach, you may want to start from the beginning of Step 2 while following one of the more cautious, alternating titration approaches.
These examples are based on common usage rates, however, there is no way to predict how many drops of molybdenum you will require or how much B2 is needed to optimize FAD levels. While some people use the indicator of neon yellow urine to signify that they are supplementing enough B2, this is not a definite indicator of functional sufficiency. It simply indicates that the body has absorbed more vitamin B2 than what it is currently capable of activating. Some people who have been functionally deficient in either nutrient for a long time may require higher doses until some of this nutrient debt is reconciled in the body.
After maintaining steady doses for at least 4 weeks, then submitting an organic acid test (OAT), we can look for markers of functional vitamin B2 sufficiency. That is a detailed topic for a future post, but for the sake of brevity, let's operate under the assumption that glutaric acid provides the most reliable information about functional vitamin B2 sufficiency in the greatest number of contexts if we were forced to choose a single marker.
While we should definitely be looking to see that this marker is not flagged high, we would preferably like to see it slightly below the 25th percentile for this marker (where the orange box meets the extended "whisker"). There is some anecdotal evidence that this percentile cutoff coincides with improved symptoms associated with functional vitamin B2 status. The example shown below just meets that criterion.

Some symptoms of a functional vitamin B2 deficiency include:
- Cracks at the corners of the mouth
- Swollen/cracked lips
- Unexplained sore throat
- Magenta-colored tongue
- Red, itchy, watery, or light-sensitive eyes
- Red, scaly patches of skin around the nose, ears, and eyelids
- Fatigue
- Anemia
- Stunted growth
- Hair loss
- Reproductive issues
- Nerve degeneration
If you experience any of these symptoms as a result of a functional vitamin B2 deficiency, as you correct the situation, you should begin to notice gradual symptom improvement commensurate to the degree of correction.
While the B12 Protocol emphasizes the importance of FAD in its context as a cofactor for MTHFR, we should also mention here that FAD (and FMN, the upstream form of activated vitamin B2) is used in many enzymes in the body, facilitating the transfer of electrons in various redox reactions. These roles are all very important to the other corners of the Trifecta, namely redox capacity and mitochondrial function.
Molybdenum deficiency symptoms can manifest as any of the functional vitamin B2 deficiency symptoms listed above, since molybdenum is required for the body to utilize vitamin B2. However, some symptoms are more specific to molybdenum and can include the following:
- Fatigue and weakness
- Mental disturbances
- Headaches
- Rapid pulse
- Rapid breathing
- Night blindness
- Nausea
- Insomnia
- Sulfur sensitivity reactions
Using Symptoms to Inform Dosing and Pace of Titration
The lists of vitamin B2 and molybdenum deficiency symptoms should be used to guide your dosage, along with other unique individual changes in how you feel and function. Note how you feel with each change - if it is positive, you may continue to test the effects of increasing the dosage until you either notice a regression in your health or fail to notice any additional change from increased intake. At that point, revert to the dose you previously tolerated and noted your last improvement from. I suggest you keep detailed, written notes in a journal, because memory can be a lousy informant!
It is our goal to maximize the transformative effects of this protocol and would be great if we could avoid any negative "growing pains", however, healing in any capacity often involves some discomfort, and we would be remiss to neglect mention of this possibility.
At Spectrum Sciences, we like to frame any negative adjustments as our body informing us of how to help us heal. In that sense, negative symptoms can be tremendously informative, though admittedly physically challenging.
If you experience a feeling like you are having a bit of an adrenaline rush that you believe may be due to protocol supplements, you may experience some relief by simply increasing potassium intake. Since this is usually a wise health choice anyhow, it makes sense to try that approach first before making any adjustments to any of the protocol supplement doses.
It is best to take symptoms and lab testing equally into consideration when deciding on how to dose Molybdenum Oil and vitamin B2.
Final Thoughts
While this blog post has not covered all of the ins and outs of taking functional vitamin B2 status to the next level with Molybdenum Oil and Vitamin B2, it covers a lot of ground.
Molybdenum is a critical component of the B12 Protocol because it is needed to activate vitamin B2 to FAD, the form used by MTHFR - often a weak link in the methylation cycle.
If you need additional help navigating the use of Molybdenum Oil and Vitamin B2 in the context of the B12 Protocol, you can arrange one-on-one coaching.
We hope you have learned something useful from this blog post. Spectrum Sciences is committed to bringing you the information that you need in order to make informed decisions about your health. We are also determined to bring you the best Vitamin B12 supplement by various means, including protocol enhancement and new product offerings.
In the next installment of this three-part series, we will cover Step 3 of the B12 Protocol: Completing the Protocol with Vitamin B12 and Folate!